

CONTACT US

MaxVP2 Handpiece

Betty Czajkowsky, M.D. SharpLight's Medical Advisor
Introduction
MaxVP2 is an IPL-DPC handpiece designed for treatment of vascular & pigmented lesions, for patients classified as Fitzpatrick skin type I-V. The device employs optical spectral filtering to optimize targeting of hemoglobin and melanin.
Treatments conducted with MaxVP2 handpiece result in clearance of the lesions, achieved by a mechanism of photothermolysis. In addition, only effective wavelengths are emitted, while applying efficient contact cooling, minimizing optional damage to darker skin tones.
Tailored Spectrum
The handpiece emits 2 bands of wavelengths, 535-680 nm and 860-1200 nm that are absorbed by melanin and hemoglobin chromophores. The 535-680 nm band targets hemoglobin absorption peaks and melanin, and is better suited for superficial lesions. The 860-1200 nm spectrum is less scattered and penetrates deeper into the skin, providing more uniform heating across the entire diameter of larger lesions. This spectrum is very efficient in enhancing treatments of deeper, wider blood vessels and is efficiently absorbed by melanin. Unnecessary light emission should always be avoided, for safety considerations.
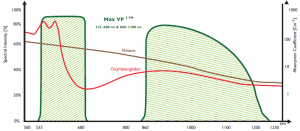
Therefore, only the abovementioned bands are emitted by the MaxVP2. The less desired 680- 860 nm band is blocked, since absorption of this excluded band by hemoglobin is insufficient, and absorption by melanin is already well assured by the emitted bands (535-860 & 860-1220 nm). We should keep in mind that absorption in the melanin might also occur by melanin concentrates in the epidermis as well. Thus, this exclusion ensures safety without compromising the results.
Therefore, this spectrum is tailored for treating superficial and deep vascular lesions, while efficiently treating superficial pigmented lesions as well.
SharpLight's unique DPC (Dynamic pulse Control) features enable selection of 3 pulse configurations, Smooth / Long / High, to accurately adjusting the treatment to the patient's specific the skin type and target characteristics.
Treatment is based on selective photothermolysis theory, according to which the minimum absorbed energy necessary to damage the targeted blood vessels / melanin should be delivered in a time comparable to the target's Thermal Relaxation Time (TRT).
Pulse Width and Peak Power
For indications that do not require treatment of the smaller, more superficial vessels and capillaries, short pulse widths and/or high peak powers should be avoided, since they lower the purpuric threshold fluence.
Contact Cooling
The melanin pigment, found in the dermal/epidermal (D/E) junction of the skin acts as competing chromospheres. In addition to decreasing the energy available to the underlying blood vessels, melanin absorption causes heating of the D/E junction that can thermally damage the epidermis. The MaxVP2 Contact Cooling provides further epidermal protection and enhances patient comfort, achieving faster treatment times with optimized results.
The MaxVP2 Contact Cooling enables selection of different Contact Cooling levels. The contact cooling should be set to LOW contact cooling in this case (5°C). Contact Cooling provides greater epidermal protection and enables delivery of save light pulses of high energy Joules/cm2. The cooling setting should be considered when treating deep or superficial vessels as described above.
Handpiece Specifications
• Technology IPL-DPC
• Tip size 1.5 cmA?
• Contact cooling Off-Low-Medium-High
• DPC Smooth / Long / High
• Pulse duration 10/ 12 / 15 / 20 / 25 msec
• Fluence 5 – 30 J/ cmA?
• Repetition Rate 0.4 Hz
• Up to 330V
Treatment Protocol
• Clearance of the lesion is usually achieved within 3 treatments.
• In each treatment, up to 3 pulses can be applied on the lesion. The first pulse is a test pulse, applying the minimal test parameter. If no response is noticed, fluence can be increased by 1 or 2 joules.
• If partial clearance is achieved, the consecutive treatment should be conducted with the same parameters which proved to be efficient.
• Interval between treatments should be 2-4 weeks.
• Pulse width selection [ms] – longer pulses are safer. For small, superficial lesions, shorter pulses are more effective (10-15 ms). For large, deeper lesions, longer pulses should be applied (≥ 20 ms).
• Fluence selection [J/cm2] – lower energies are safer. For small, superficial lesions, energy levels must be selected with caution and should not be too high (15-19 J). For large, deeper lesions, higher energy should be delivered (20-25 J).
• DPC type – Smooth Pulse is recommended for accuracy considerations. Working with other DPC types (high / long) should be confined to rare cases in which the practitioner is highly skilled and the ms are very long. Immediate responses – When treating vascular lesions, an immediate clearance / brightening is expected. When treating pigmented lesions, an immediate response of lesion darkening is expected.
Study cases
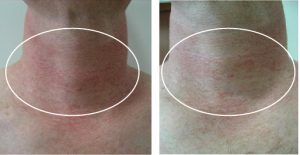
1. Caucasian female, 45 years old, skin type II, with familiar poikiloderma predisposition on her neck. In the clinic of Dr. Kaplan, plastic surgeon in Israel, she received 2 treatments, one month apart with SharpLight's OmniMax hand piece VP2.
Parameters with efficient result in vessel coagulation were:
• 1 tx – DVL- DPC Long- pulse duration 20 ms- fluence 18 J/cm2
• 2 tx- LVL- DPC Long- pulse duration 20 ms- fluence 22 J/cm2
Before After second treatment

2. Caucasian male, 50 years old, with broken capillaries in his nose because of sun exposure without protection. In the clinic of Dr. Shohad, plastic surgeon in Israel, he received one treatment.
• 1 tx – DVL- DPC Long- pulse duration 15 ms- fluence 15 J/cm2
Before After 1 treatment

3. Caucasian female, 55 years old, skin type II, with familiar poikiloderma predisposition on her neck. In the clinic of Dr. Kaplan, plastic surgeon in Israel, she received 1 treatment.
Before After 1 treatment
4. Caucasian male, 65 years old, skin type II, with familiar with broken capillaries in his nose because of aging. In the clinic at SharpLight, Dr. Czajkowsky, Medical Advisor of the company, in Israel, he received 3 treatments.
• 1 tx – DVL- DPC Long- pulse duration 15 ms- fluence 14 J/cm2
• 2 tx – DVL- DPC Long- pulse duration 12 ms- fluence 18 J/cm2
• 3 tx- LVL- DPC Long- pulse duration 10 ms fluence 22 J/cm2
Before After 3rd treatment

Recommendations
• If the lesion is smaller than the handpiece tip, use of the provided templates is recommended. Place the template on the lesion in order to border the radiant skin area and minimize unnecessary light absorption by the surrounding skin tissue.
• The patient should avoid exposure of the treated area to the sun for 14 days following the treatment. If sun exposure cannot be avoided, the patient must apply sun-block rated as at least 30 SPF during the following 14 days.
• Darker skin tones should be treated with greater caution – longer pulses and lower energies should be employed.
Results and Conclusion
The device employs optical spectral filtering to optimize targeting of hemoglobin and melanin. Treatments conducted with MaxVP2 handpiece result in clearance of the lesions, achieved by a mechanism of photothermolysis. In addition, only effective wavelengths are emitted, while applying efficient contact cooling, minimizing damage to darker skin tones.
When using a handpiece for treating superficial vascular and pigmented lesions and deeper blood vessels, it is essential to tailor the spectrum in order to achieve an efficient and safe treatment. The spectral ranges are efficient in treating vascular and pigmented lesions. The blocked spectrum 680-860 nm enhances the epidermal protection. The fast efficacy of the results (90%) and the lack of undesirable secondary effects resulted in high satisfaction.
References
1. Bjerring P, Christiansen K, Troilius A. Intense pulsed light source for the treatment of dye laser resistant port-wine stains. J Cosmet Laser Ther 2003; 5(1):7-13.
2. Adatto MA, Luc-Levy J, Mordon S. Efficacy of a novel intense pulsed light system for the treatment of port wine stains. J Cosmet Laser Ther 2010; 12(2):54-60.
3. Ho WS, Ying SY, Chan PC, Chan HH. Treatment of port wine stains with intense pulsed light: a prospective study. Dermatol Surg 2004; 30(6):887-890; discussion 890-881.
4. Reynolds N, Exley J, Hills S, Falder S, Duff C, Kenealy J. The role of the Lumina intense pulsed light system in the treatment of port wine stains–a case controlled study. Br J Plast Surg 2005; 58(7):968-980.
5. Nymann P, Hedelund L, Haedersdal M. Intense pulsed light vs. long-pulsed dye laser treatment of telangiectasia after radiotherapy for breast cancer: a randomized split-lesion trial of two different treatments. Br J Dermatol 2009; 160(6):1237-1241.
6. Wenzel SM, Hohenleutner U, Landthaler M. Progressive dis seminated essential telangiectasia and erythrosis interfollicularis colli as examples for successful treatment with a highintensity flashlamp. Dermatology 2008; 217(3):286-290.
7. Schroeter CA, Haaf-von Below S, Neumann HA. Effective treatment of rosaceausing intense pulsed light systems. Dermatol Surg 2005; 31(10):1285-1289.
8. Papageorgiou P, Clayton W, Norwood S, Chopra S, Rustin M. Treatment of rosacea with intense pulsed light: significant improvement and long-lasting results. Br J Dermatol 2008; 159(3):628-632.
9. Garden JM, Polla LL, Tan OT. The treatment of port-wine stains by the pulsed dye laser. Analysis of pulse duration and long-term therapy. Arch Dermatol 1988; 124(6):889-896.
10. Bernstein EF, Lee J, Lowery J, Brown DB, Geronemus R, Lask G, Hsia J. Treatment of spider veins with the 595 nm pulsed-dye laser. J Am Acad Dermatol 1998; 39(5 Pt1):746-750.
11. Yang MU, Yaroslavsky AN, Farinelli WA, Flotte TJ, Rius- Diaz F, Tsao SS, Anderson RR. Longpulsed neodymium: yttrium-aluminum-garnet laser treatment for port-wine stains. J Am Acad Dermatol 2005; 52(3 Pt 1):480-490.
Kimel S, Svaasand LO, Cao D, Hammer-Wilson MJ, Nelson JS. Vascular response to laser photothermolysis as a function of .169-160:)2(30 ;pulse duration, vessel type, and diameter: implications for port wine stain laser therapy. Lasers Surg Med2002
12. Fiskerstrand EJ, Svaasand LO, Kopstad G, Ryggen K, Aase S. Photothermally induced vesselwall necrosis after pulsed dye laser treatment: lack of response in port-wine stains with small sized or deeply located vessels. J Invest Dermatol1996; 107(5):671-675.
13. Woo SH, Ahn HH, Kim SN, Kye YC. Treatment of vascular skin lesions with the variable-pulse 595 nm pulsed dye laser. Dermatol Surg 2006; 32(1):41-48.
14. Faurschou A, Togsverd-Bo K, Zachariae C, Haedersdal M. Pulsed dye laser vs. intense pulsed light for port-wine stains: a randomized side-by-side trial with blinded response evaluation. Br J Dermatol 2009; 160(2):359-364.
15. Jorgensen GF, Hedelund L, Haedersdal M. Long-pulsed dye laser versus intense pulsed light for photodamaged skin: a randomized split-face trial with blinded response evaluation. Lasers Surg Med 2008; 40(5):293-299.
16. Anderson RR, Parrish JA. Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science 1983; 220(4596):524-527
17. New Optimized Light Source for Treatment of Vascular Lesions of the Skin E. Victor Ross, MD1; Emil A. Tanghetti, MD2; David B. Vasily, MD3; Robert A. Weiss, MD4; James J. Childs, PhD5; Andrei Erofeev, PhD5; Mikhail Z. Smirnov, PhD5; and Gregory B. Altshuler, PhD, ScD5
SharpLight Technologies Ltd. is an expert in the design and manufacture of cutting edge aesthetic devices. We offer a wide variety of stand-alone & multi-technology solutions that deliver superior clinical results. READ MORE



