

CONTACT US

IR Hand piece for Face and Body Skin Tightening: a Hot Topic Utilizing Deep Dermal Heating

Dr. Betty Czajkowsky, M.D.
SharpLight Technologies Medical Advisor
INTRODUCTION
A non coherent, selectively filtered infrared device emitting infrared light in multi-second cycles has been developed with the intention to provide dermal heating.
Water, as the target chromospheres, allows uniform heating of the targeted skin tissue volume. A tailored wavelength spectrum from 850 to 1,750 nm on one hand sufficiently absorbed by intracellular and extracellular water yet allows a penetration depth of 1-2 mm into the skin which is ideal for targeting the reticular dermis.
A multi second exposure is used with sufficient energy to create the desired combination of time and temperature for collagen contraction. The epidermis is protected through contact cooling. This allows for heating of the treated tissue without epidermal damage.
Collagen is a polymer that exists as a triple helix with chains held together by hydrogen bonds. These molecules are aggregated and organized as fibrils with tensile properties attributable to intermolecular cross-links. When collagen is denatured by heat, the intra molecular hydrogen bonds rupture and the triple helices "unwind to produce a gel of random-coil molecules." Tissue tension in human skin increases because, although the fibers become shorter, the heat-stable cross-links between molecules are maintained, thus increasing the rubber-elastic properties of the collagen polymer. The heat-modified tissues then undergo remodeling associated with fibroplasias and new collagen deposition. When denaturation is complete, further increases in temperature result in additional fiber shortening, probably because of peptide bond hydrolysis.
The mechanism of collagen shrinkage has been described in detail. The temperature at which collagen shrinkage occurs is often quoted as 65° C. According to this equation, shrinkage of collagen depends on time, as well as temperature, and collagen contraction occurs at a variety of time-temperature combinations rather than at a specific temperature. That said, it has been suggested that for millisecond exposures, collagen shrinkage will occur only at temperatures exceeding 85° C, whereas for exposures of several seconds, shrinkage will occur at 60° to 65° C. Collagen contraction begins to occur at approximately 55°C. This is caused by the spread of heat to the deeper reticular dermis.
In contrast to radiofrequency, the IR infrared spectrum is both predictable and easily understood based on the known coefficients to the target chromospheres of water. SLT uses a unique spectral profile between 850nm to 1750nm. This IR source outputs from 5J/cm2 to 80 J/cm2, based on the area being treated, resulting in heating at depths from 1-3mm. The epidermal temperature is kept at a safe level of below 40°C by an integrated thermoelectrically cooled sapphire window which also assists in maintaining patient comfort during the treatment.
This unique IR spectrum creates a "dual clinical effect" of immediate skin tightening together with long term new dermal collagen formation. The primary function of this device is tightening of skin laxity in parts of the body such as the face cheeks and neck area and body areas as arms, abdomen, buttocks, tights, etc. Pain levels are reported to be well tolerated. The device is also intended for smoothing of facial wrinkles as part of the neocollagenesis phenomenon.
MATERIALS AND METHODS
An IR halogen lamp hand piece for the SharpLight's Aesthetic Station has been tested on twenty (20) volunteers, all females, aged between 45 and 65, with various degrees of lax skin in the face, neck, arms, abdomen, hips, upper buttocks and thighs. The twenty (20) volunteers received eight (8) treatments, once a week for two month. Time of each treatment session varies depending on the area treated: face and neck around 20 minutes while body areas like abdomen or both thighs around 30 minutes. Standardized photographs were taken at baseline, after the 4th treatment and after the 8th treatment. One month follow-up visit was also assessed. Patient satisfaction scores were recorded at the final visit. Each session's data was recorded for future evaluation.
Hand pieces came in 2 spot sizes: 3.4 and 6.4 cmA? for more precise full contact skin/waveguide and the Fluence is up to 80 J/ cm2.
SharpLight offers a unique addition which is the Fractional window pane 7×3 that can be added to the wave guide hand piece in order to lower diffuse the heat making the treatment more comfortable and less painful over bone and teeth areas.
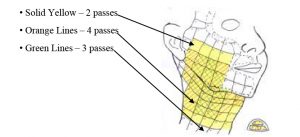
It quickly became clear that a greater amount of collagen denaturation can be induced with multiple passes, 4-5 times, using lower energy levels.
Passes are performed over the entire designated treatment area, with additional passes over the areas of more concern. To soften the nasolabial fold, an extra strip of 2-3 cm in the pre-auricular area is treated. To obtain eyebrow elevation, extra passes on the upper portion of the forehead and temples are given. The neck is treated directly in the sub mental area. At these settings, the procedure is very well tolerated.
It is recommended to use lower fluences over bony areas such as the forehead. These areas have been found to be especially sensitive in many patients and treatment of this area is often avoided.
On certain more sensitive areas the fluencies are usually lowered same due to discomfort. If the patient mentions an immediate burning sensation after the pulse, ice is applied immediately to prevent tissue burns. This is usually the result of incomplete skin contact with the cooled sapphire window during IR application. Immediately after treatment, diffused mild erythema with
slight edema is evident in the area, but it usually fades within 1 hour. Occasionally, small superficial burns develop after treatment if proper contact with the skin is not maintained. With the appropriate aftercare, these superficial burns heal uneventfully.
Physicians are currently using IR in two distinct treatment approaches. One method is to use the highest tolerable fluences. The second method is to use lower fluences with a higher number of pulses in concentrated areas. This approach has shown results in lifting of the eyebrows in addition to the lower face results. What has been reported thus far is that patients who respond best are those with sub mental laxity and jowls.
In this comparative conclusion, IR is effective for the following reasons: 1) Greater safety profile, more predictable. 2) Equal or near equal in dermal heating capability. 3) Superior epidermal cooling method 4) Scalable platform.
Patient selection: Best results are often seen in patients with a minimum of excess fat in the area of concern and with thinner skin that is easily moved with a gentle touch Patient should be able to tolerate the treatment with no more than a moderate level of discomfort.
Treatments are commonly performed once a week but every 2 weeks is also effective but not as fast visible results. Maintenance should be done every 6 month to keep the up the skin tightening.
The IR hand piece

3 treatment phases
Full cycle lasts approximately 10 seconds:
• Pre-Cooling through sapphire window regulated at around 10° C
• Dermal heating with infrared light with simultaneous epidermal cooling
• Post-Cooling through sapphire window regulated at around 10° C

Pre-cooling IR pulse Post cooling
Treatment Areas
RESULTS
At 1 month after the last treatment, 70% of the subjects exhibited moderate to significant improvement in skin laxity and skin texture on the face, neck, arms, abdomen, buttocks and thighs.
Patients reported high overall satisfaction with the treatment. Objective and subjective evidence of face and neck skin tightening, less wrinkles and folds and more skin glowing; in the cheeks and around the eyes were highly appreciated. Body areas also showed high improvement in skin sagginess.
No serious complications were recorded and all redness was temporary and did not require any special treatment, only moisturizers.
It is interesting to note that patient sensitive to heat and pain was reduced by the addition of a Fractional window pane. This allowed a more comfortable treatment with the use of higher
fluence and more passes, leading to an improved end result. For patients with facial textural damage, sun or age pigmented lesions and broken capillaries, the combination of ILP monthly treatments together with IR treatments, significantly added to the younger and healthier final skin appearance.
Patient satisfaction scores:
| Very satisfied | 70 % |
| Satisfied | 20 % |
| Not satisfied | 10% |
B/A PHOTOS
Before After 6 treatments

Before After 10 treatments

CONCLUSIONS
Periodic maintenance sessions may be administered as required or desired by each individual patient.
The availability of this new IR hand piece significantly enhances the capabilities of the SLT Aesthetic Station, broadening its clinical indications to include skin tightening on all body areas.
The new IR hand piece has demonstrated to be highly effective and safe for non-invasive face and body skin tightening. Quantitative and qualitative results were documented in the treatment of face and neck skin laxity and improved texture and of sagging of arms abdomen, thighs and buttocks. Very high patient satisfaction was achieved. The procedure is easy to apply, involves no discomfort to the patient and requires no downtime whatsoever.
REFERENCES
Watson RE, Parry EJ, Humphries JD, Jones CJ, Polson DW, Kielty CM, Griffiths CE (1998) Fibrillin microfibrils are reduced in skin exhibiting striae distensae. Br J Dermatol 138:931-937
Ghersetich I, Kopera D, Levy JL, Trelles MA (2006) The efficacy of a new powerful infrared light system for the treatment of cosmetic dermatological disorders. Intl. Congress of ESLAS, Graz, Austria
Trelles MA, Mordon S (2006) Cutaneous effects compared between higher fluence with fewer treatments and lower fluence with more treatments in a combined IR laser/radio frequency system. J Cosmetic Laser Ther 8:177-183
Effects Achieved on Stretch Marks by a Nonfractional Broadband Infrared Light System Treatment. M. A. Trelles1, J. L. Levy2 and I. Ghersetich3
Treatment of skin laxity of the lower face and neck in older individuals with a broad- spectrum infrared light device. David J. Goldberg 1,2†,, Mussarrat Hussain1, Amon Fazeli1 and Alexander L. Berlin1
Dierickx CC, Altshuler GA, Erofeev A, Smirnov M, Childs J, Yaroslavsky I. Deep dermal optical/island damage as a novel approach to skin tightening. Lasers Surg Med 2006;S18:80.
Narukar V. Full thickness permanent scars from bulk heating using an infrared light source. Lasers Surg Med2006;S18:96.
Ruiz-Esparza J. Near painless, nonablative, immediate skin contraction induced by low-fluence irradiation with new nfrared device: A report of 25 patients. Dermatol Surg. 2006;32:601-10.
Lee M-WC. Comparison of radiofrequency vs. 1100-1800 nm infrared light for skin laxity. Am Soc Derm Surg Abstracts, Atlanta, GA; October 27, 2005.
Zelickson B, Ross V, Kist D, Counters J, Davenport S, Spooner G. Ultrastructural effects of an infrared handpiece on forehead and abdominal skin. Dermatol Surg.
2006;32:897-901.
Kopera D, Smolle J, Kaddu S, Kerl H. Non-ablative Laser Treatment of Wrinkles: Meeting the Objective? Assessment by 25 Dermatologists. Brit J Dermatol 2004, 150: 936-939.
Sadick NS. Nonsurgical approaches to skin tightening. Cosmetic Dermatology 2006;19: 473-477.
Ruiz-Esparza J. Painless, nonablative, immediate skin contraction induced by low-fluence irradiation with new infrared device: a report of25 patients. Dermatol Surg 2006;32:601-610
Bunin L, Carniol P. Cervical facial skin tightening with an infrared device. Facial Plast Surg Clin North Am 2007;15:179-184.
Zelickson B, Ross V, Kist D, Counters J, Davenport S, Spooner G. Ultrastructural effects of an infrared handpiece on forehead and abdominal skin. Dermatol Surg 2006;32:897-901.
Taub A, Battle EF, Nikolaidis G. Multi center clinical perspective on a broadband infrared light device for skin tightening. J Drugs Dermatol2006;5:771-758.
Chua S, Ang P, Khoo L, Goh C. Nonablative infrared skin tightening in type IV to V Asian skin: a prospective clinical study. Dermatol Surg2007;33:146-151.
Goldberg D, Hussain M, Fazeli A, Berlin A. Treatment of skin laxity of the lower face and neck in older individuals with a broad-spectrum infrared light device. J Cosmet Laser Ther 2007;9:35-40.
Alexiades-Armenakas M. Laser skin tightening: non-surgical alternative to the face lift. J Drugs Dermatol 2006;5:295-296.
Montagna W, Carlisle K. Structural changes in ageing skin. Br J Dermatol 1990;122 (Suppl 35):61-70.
Dierickx CC. The role of deep heating for noninvasive skin rejuvenation. Lasers Surg Med 2006;38:799-807.
Zelickson B, Ross V, Kist D, et al. Ultrastructural effects of an infrared handpiece on forehead and abdominal skin. Dermatol Surg 2006;32:897-901.
Ruiz-Esparza J. Near [corrected] painless, nonablative, immediate skin contraction induced by low-fluence irradiation with new infrared device: A report of 25 patients. Dermatol Surg 2006;32(5):601-610.
Chua SH, Ang P, Khoo LS, Goh CL. Nonablative infrared skin tightening in Type IV to V Asian skin: A prospective clinical study. Dermatol Surg 2007;33:146-151.
Yu C, Shek S, Yeung CK, Kono T, Chan HH. Combined infrared light and bipolar radiofrequency for skin tightening in Asians. Lasers Surg Med 2007;S19:65.
Taub AF, Battle EF, Nikolaidis G. Multicenter clinical perspectives on a broadband infrared light device for skin tightening. J Drugs Dermatol. 2006;5(8):771-8.
Carniol PJ, Dzopa N, Fernandes N, Carniol ET, Renzi AS. Facial skin tightening with an 1100-1800 nm infrared device. J Cosmet Laser Ther. 2008;10:67-71.
Kameyama K. Histological and clinical studies on the effects of low to medium level
infrared light therapy on human and mouse skin. J Drugs Dermatol. 2008;7(3):230–5.
SharpLight Technologies Ltd. is an expert in the design and manufacture of cutting edge aesthetic devices. We offer a wide variety of stand-alone & multi-technology solutions that deliver superior clinical results. READ MORE



